The CARE Act is a paradigm shift
CARE is a compassionate civil court process that provides participants with a clinically appropriate, community-based set of services and supports that are culturally and linguistically competent. Individualized CARE plans can initially be structured to last up to 12 months, and can be extended for an additional 12 months as necessary. CARE plans ensure participants receive a broad range of necessary services, including short-term stabilization medications, wellness and recovery supports, and connection to other social services such as housing. Housing will be an important component of many successful CARE plans —we recognize that finding stability and staying connected to treatment, even with the proper supports, is next to impossible while living outdoors, in a tent or a vehicle.
The CARE process is an upstream diversion to prevent more restrictive conservatorships or incarceration; this is based on evidence which demonstrates that many people can stabilize, begin healing, and exit homelessness in less restrictive, community-based care settings. With advances in treatment models, new longer-acting antipsychotic treatments, and the right clinical team and housing, participants who have historically suffered tremendously on the streets or during avoidable incarceration can be successfully stabilized and supported in the community.
CARE is not for everyone experiencing homelessness or mental illness; rather it focuses on people with schizophrenia spectrum or other psychotic disorders who meet specific criteria – before they get arrested and committed to a State Hospital or become so impaired that they end up in a Lanterman-Petris-Short (LPS) Mental Health Conservatorship. CARE may also be an appropriate next step after a short-term involuntary hospital hold (either 72 hours/5150 or 14 days/5250) or for those who can be safely diverted from certain criminal proceedings. Although homelessness has many faces in California, among the most tragic is the face of the sickest who suffer from treatable mental health conditions—this proposal aims to connect these individuals to effective treatment and support, mapping a path to long-term recovery. CARE will help thousands of Californians on their journey to sustained wellness.
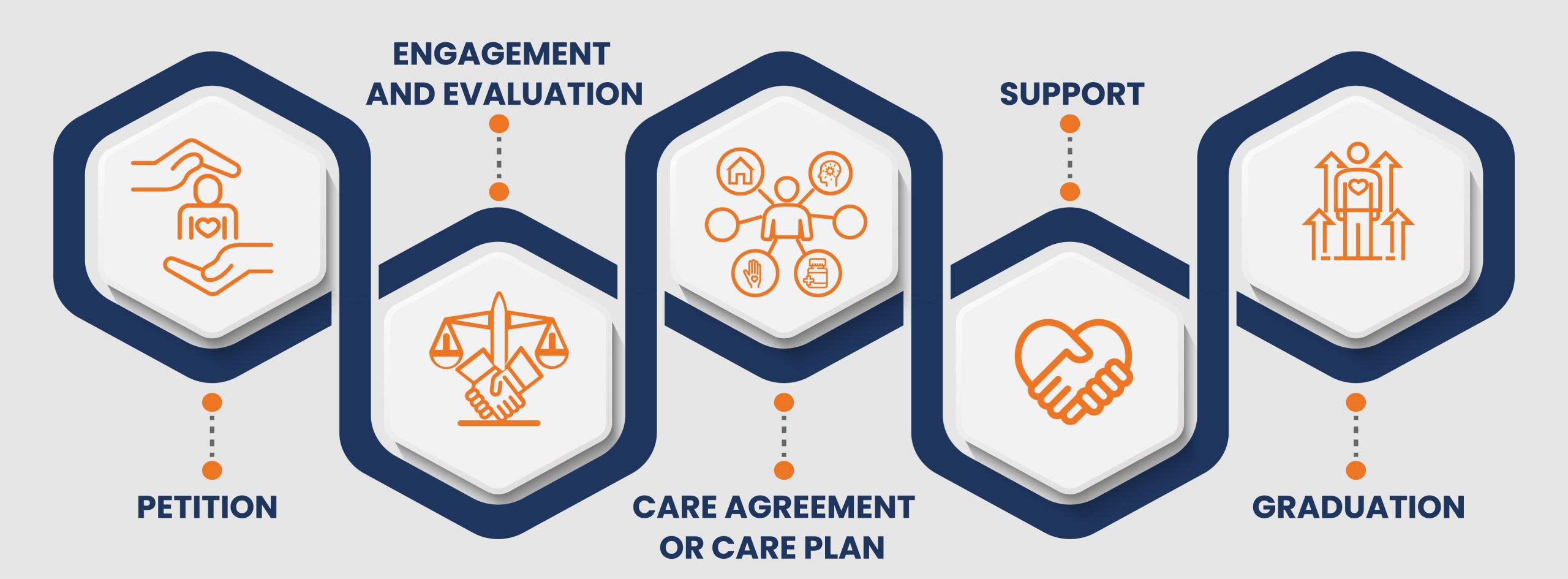
Supporting a path to recovery and self-sufficiency is core to CARE. CARE engagement begins with a petition to the Court from a wide range of individuals, including care providers, family members, first responders, and others specified in the CARE Act. Participants will be provided with legal counsel and a voluntary supporter chosen by the participant, if desired, in addition to their full clinical team. The role of the supporter is to help the participant understand, consider, and communicate decisions, giving the participant the tools to make self-directed choices to the greatest extent possible. The CARE plan ensures that appropriate supports and services are identified, coordinated, and focused on the individual needs of the participant. This includes coordination of services such as clinical treatment and housing, which are often disconnected. The creation of a Psychiatric Advance Directive will help protect the autonomy of participants by legally documenting their treatment preferences in advance of a potential future mental health crisis.
Accountability in CARE goes both ways
If a participant cannot successfully complete a CARE plan, the Court may utilize existing authority under the LPS Act to ensure the participant’s safety. If the respondent was provided all the services and supports in the CARE plan, the participant’s failure to complete a CARE plan will be considered in any subsequent hearings under the LPS Act that occur within 6 months of the termination of the CARE plan, and shall create a presumption at that hearing that the respondent needs additional intervention beyond the supports and services provided by the CARE plan.
CARE will also hold local governments accountable for providing care to the people who need it, using the variety of robust funding streams available to counties today. These funding sources include over $10 billion annually for behavioral health care, including the Mental Health Services Act and behavioral health realignment funds. Various housing and clinical residential placements are also available to cities and counties, including over $15 billion in state funding that has been made available over the last two years to address homelessness. CARE Court participants will also be prioritized for any appropriate bridge housing funded by the Behavioral Health Bridge Housing program, which provides $1.5 billion in funding for housing and housing support services. If local governments do not meet their specified responsibilities under the court-ordered CARE plans, the Court will have the ability to order sanctions and, in extreme cases, appoint an agent to ensure services are provided.